BTS #11 Jason Miller DACM on Chinese Medicine, Cannabis, Cancer
In this behind-the-scenes (BTS) episode we speak with Dr. Jason Miller, an expert in traditional Chinese medicine with a focus on the treatment of cancer. In this conversation we explore how Dr. Miller conceptualizes Cannabis in relation to other medicinal plants, historical uses of Cannabis in Chinese medicine, the promise and limitations of Cannabis as a medicine, his experience with Cannabis as a cancer treatment, bridging the worlds of eastern and western medicine, and much more!
Enjoy, and stay curious!
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
BTS #10 Steve Albarran CEO of Confident Cannabis on Transparency, Lessons from Big Data, Chemotypes, Market Trends
In this behind-the-scenes (BTS) episode we sit down with Steve Albarran, the CEO of Confident Cannabis, a technology company that has been working to bring transparency to the Cannabis industry through various software solutions that allow labs, producers, and consumers to share product information and test results seamlessly. In this conversation we explore how Confident Cannabis got started and where the company is headed, insights that can be taken from the data that Confident Cannabis has managed, lessons that users have gleaned from Confident Cannabis’ chemotype visualization tool called Connect, trends in the marketplace, and much more.
I hope you enjoy. Stay curious, and take it easy.
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
BTS #08 Wyeth Callaway PhD on Extraction Technology, Cannabis Essential Oils, Quality Control
In this behind-the-scenes (BTS) interview we speak with Dr. Wyeth Callaway (aka @DrJackHughes), an organic chemist currently working in the Cannabis industry. In this interview we discuss a wide range of Cannabis extraction related topics including commonly used extraction technologies, the pros and cons of different forms of extraction, unique considerations when extracting Cannabis essential oils, how to manage the quality of extracts, and much more!
I hope you enjoy our conversation! Stay curious and take it easy.
For more content visit www.CACPodcast.com
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
BTS #05 Ethan Russo MD on CBD, Entourage Effects, the Endocannabinoid System and Cannabinoid Pharmaceuticals
In this behind-the-scenes (BTS) episode we talk with the world renowned Cannabis and cannabinoid researcher, Dr. Ethan Russo, to discuss a host of topics like the alleged toxicity of CBD, the research evidence for entourage effects, how to think about the endocannabinoid system, how Cannabis based pharmaceuticals are developed and more! We packed a lot of good conversation in this relatively short conversation. Enjoy and stay curious!
P.S. This will be our last episode until after the Christmas and New Year holidays, but we will be back and ready to go first thing at the turn of the New Year. Stay safe and happy holidays!
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
BTS #04 Kevin Spelman PhD on the Endocannabinoid System, Plant Synergies, and Dietary Supplement Research
In this behind-the-scenes (BTS) interview, we sit down with Kevin Spelman, PhD, a molecular biologist and medicinal plant expert that has spent time studying the endocannabinoid system (ECS) and how medicinal plants affect the ECS. In this interview we discuss how to think about the “entourage effect”, biases in science against medicinal plant research, the safety and efficacy of medicinal plants and dietary supplements, misconceptions about Cannabis, and much more! Stemming from the release of episodes 4 and 5 of the podcast where we explore the concept of Cannabis as a medicine, this interview contains a lot of content that got cut from those episodes for time that many of you will likely enjoy.
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
#05 Cannabis as Medicine – Part Two: Medical Research and Clinical Outcomes
Episode Description: Continuing from our previous episode where we began exploring the idea of Cannabis as medicine, in this episode we dive into exploring how medical claims are derived, what it takes to develop a Cannabis-based drug in the United States, and what outcomes health care professionals are seeing in their patients that are using Cannabis as a medicine.
TRANSCRIPT
You’re listening to the Curious About Cannabis Podcast
Before we get started let me share a little disclaimer here. In this episode we are going to be discussing the medical uses of Cannabis. All of the information I present to you in this podcast is for education and entertainment purposes only and should not be considered medical advice. Never make decisions about your health based on anything you hear me or any other podcast host talk about. I’m simply sharing information that I’ve collected from talking with professionals with relevant experience or from research studies that are available. But I’m not a doctor, and you should always get your medical advice from a licensed health care professional. Now with that out of the way, let’s move on.
n
[INTRO SEGMENT]
n
In the previous episode of the podcast we began exploring the concept of Cannabis as medicine. We looked at many of the ways in which Cannabis has been used as a medicine in the past, and some ways in which Cannabis based pharmaceuticals are being used as medicines today. Picking up where we left off, I wanted to explore the ways in which medical claims are derived. How do we determine that something is a medicine? And what results are clinicians seeing in their patients that are using Cannabis?
n
[INTRO MUSIC]
n
Hey everybody, this is Jason Wilson with the Curious About Cannabis Podcast, thanks so much for tuning in once again.
n
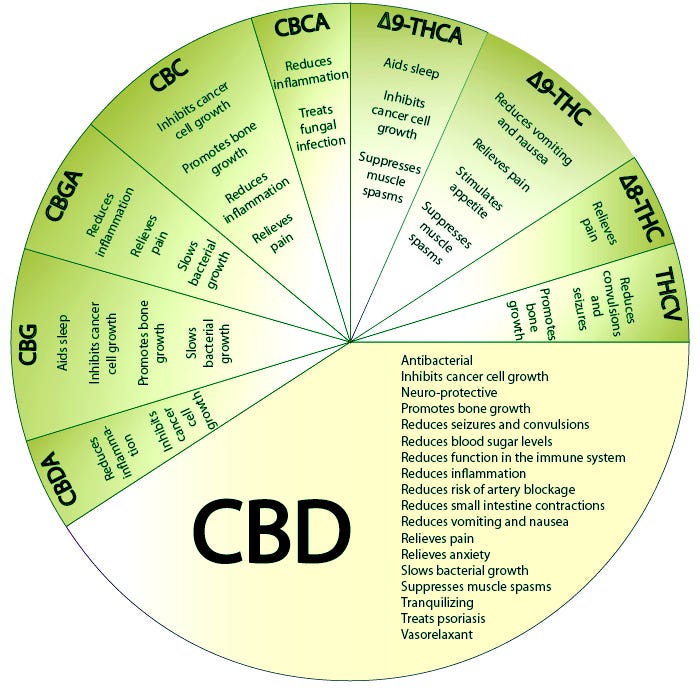
As we covered in the previous episode, there are a lot of medical claims swirling around Cannabis. If you go into just about any Cannabis dispensary, you are likely to see posters on the wall indicating the myriad of different chemicals in Cannabis and their supposed effects.[1] [2] However, many times these kinds of charts are built off of very simple, pre-clinical research data, that may not have any relevance in a real-life Cannabis use scenario.
n
How are medical claims derived?
n
So, how are medical claims derived?
n
There are several forms of medical research of varying degrees of quality.[3] On one end of the spectrum are anecdotal reports – these are basically eye-witness testimonies from a single person or small group of people. Up from that you have case studies, usually written by a professional describing an incident in detail. Moving along, there are observational studies, where a health care professional watches a patient engage in an activity and records the outcomes. On the other far end of the spectrum is the gold standard of randomized controlled trials.[4]
n
When a drug is being developed, typically the first way it is studied is through in vitro research.[5] In vitro studies are laboratory studies performed in test tubes or petri dishes. In vitro literally means, “in glass”.
n
[JUSTIN FISCHEDICK]
n
This is Justin Fischedick. Justin is a natural products researcher that studies the activity of the chemical constituents of plants, including Cannabis.
n
[JUSTIN FISCHEDICK]
n
Then there are in vivo studies, which are in living animals.[6]
n
[JUSTIN FISCHEDICK]
n
But there are limitations to each of these types of studies, and the results of an in vitro study or an in vivo animal study cannot always be easily extrapolated to real-life human clinical situations.[7]
n
[JUSTIN FISCHEDICK]
n
I had a conversation with cellular and molecular biologist, Dr. Anthony Smith, about this issue regarding the limitations of animal studies.[8]
n
[ANTHONY SMITH]
n
A lot of Cannabis research has, up to a point, been primarily in vitro and in vivo rodent studies, but very few research projects with Cannabis have crossed into the world of placebo controlled double blind clinical trials with large patient populations, and many politicians and regulatory bodies continue to claim that because of this lack of clinical trial data, herbal Cannabis or Cannabis products cannot be deemed safe or a viable medicine for a condition.
n
Let’s break this phrase down. “Placebo controlled” refers to the fact that a compound is given to some of the patients in a trial which is intended to have no effect. In general, it is expected that if something is a candidate to be considered a medicine, it needs to perform better than a placebo. It can be difficult to adequately utilize a placebo in a THC-rich Cannabis study. Because THC has such distinct effects, it is pretty difficult to fool people into thinking they got the drug when they actually did not. This is referred to as “incomplete blinding” because the patients are not truly blinded to whether they received the drug or not. The gold standard for clinical trials is for a study to be “double blind”.
n
“Double blind” refers to the idea that both the clinician performing the study, and the patients participating in the study, are blind to whether they received the research drug, or the placebo. This is important because there are various biases that can enter a study if the physician knows who has had the placebo or not, and likewise, patients may react differently in a study if they know they are receiving a placebo – although some modern research is beginning to call this idea into question.
n
Lastly, large sample sizes are required in order to understand whether the results of a clinical trial are representative of a larger population.[9] A study that only examines the response of a couple dozen or even a couple hundred people is really small, and can’t really represent the hundreds of millions of people living in the United States, much less the billions of people living in the world.
n
There’s also the issue of repeatability that is worth mentioning. Even if a research study is placebo-controlled and double blinded with a good sample size – it is still important that the study be replicated by another set of researchers, in another location, with a different population of people. Research findings are much more robust when they have been repeated.[10] There is always the chance that there are some variables unaccounted for in a study that could explain the results differently than what the researchers were focused on.
n
When trying to interpret medical research, there is also the issue of deciphering what the clinical studies are trying to measure, and whether the significant effects that are identified in a study are relevant in a real-life clinical setting. This is the issue of statistical significance vs clinical significance.[11] Statistical significance is a measure of the likelihood that a result is not due to pure chance. Whereas clinical significance is a measure of the practical significance of a treatment in a clinical setting. Basically, just because a research study determines that something exhibits an effect that is statistically significant, it doesn’t mean that the effect will end up being significant in any practical sense when someone consumes that thing.
n
There is another similar issue also facing drug development and medical research, and that’s the battle between efficacy research and effectiveness research.[12]
n
[JASON MILLER]
n
So we’ve established that there are a lot of different ways to study medicine, and the results of some of these studies are not necessarily straightforward to interpret.
n
[ETHAN RUSSO]
n
All of these nuance details about research are important when it comes to the development of Cannabis based pharmaceuticals. To get a drug approved as a medicine in the United States, a company has to present lots of data that shows that the drug, and not a placebo, provide an intended therapeutic effect for a particular condition or set of conditions.[13] That takes a lot of time, a lot of energy, and a lot of money.
n
[ETHAN RUSSO]
n
Sativex, or Nabiximols as it is also known, is a particularly interesting drug to focus our attention on. Sativex is a mouth spray that consists of a standardized Cannabis extract with a 1:1 ratio of CBD to THC.[14] Unlike Epidiolex[15], which is often criticized for being an isolated cannabinoid drug like Marinol[16] – Sativex consists of a wide diversity of plant compounds extracted from Cannabis. This means that the clinical data on Sativex is likely to be more relevant when thinking about the therapeutic potential of herbal Cannabis or Cannabis extracts, than research on isolated THC, like Marinol, or CBD, like Epidiolex.
n
[ETHAN RUSSO]
n
Dr. Russo makes a great point here. Just because cannabinoid and Cannabis-based pharmaceuticals are being developed, it doesn’t mean that herbal Cannabis and the use of Cannabis extracts is going away anytime soon.
n
And in fact, many people tend to prefer the use of herbal Cannabis or Cannabis extracts for a number of reasons. Sometimes it’s efficacy related, but sometimes it’s cost related. Pharmaceuticals can be extremely expensive.[17] When you can grow a plant at home and can easily make your own extract with as good or better efficacy than a pharmaceutical, it’s pretty hard to justify going the pharmaceutical route. However, pharmaceuticals are standardized and very consistent batch to batch. It’s possible that trying to treat a condition with homegrown Cannabis or black market (or even legal medical or recreational) Cannabis may not provide consistent outcomes because the products’ chemistry will be different batch to batch.
n
Unfortunately, there is really not much research available regarding herbal Cannabis or Cannabis extracts. This is for multiple reasons. One reason is that research tends to happen with products that can be patented. So, there is not a huge financial incentive to do expensive research on herbal Cannabis or unstandardized Cannabis extracts. Another issue is that Cannabis flower and extracts are very diverse and inconsistent in their chemistry batch to batch.
n
What are clinicians seeing in patients using Cannabis?
n
However, despite all of these issues, clinicians around the US are noticing striking results in many patients.
n
[JANNA CHAMPAGNE]
n
[JAMES TAYLOR]
n
All of this positive benefit that some of these health care professionals are seeing does not mean that Cannabis is without risks. For an in-depth review of the risks associated with Cannabis use, I recommend listening to the first three episodes of this season where we explored the question, “Is Cannabis Safe?”.
n
Cannabis can interact with other medications and it’s not for every person or every condition.
n
[JASON MILLER]
n
So despite some of the miraculous claims about Cannabis – it’s not a cure-all, and some of the claims made by advocates are overhyped. However, other clinicians I spoke with shared additional stories of the successes of the medical use of Cannabis – which begs a question – just how much evidence is required before Cannabis, or any other natural product, can be accepted as an effective medicine?
n
We’ve discussed that the gold standard of medical research is considered to be the randomized controlled trial – but it’s an extremely expensive process to get something through the drug approval process in the United States.[18] Because this process is so expensive, it is rare for a company to spend the millions, or sometimes billions, of dollars required to study a natural product alone that they cannot patent and capitalize on later. Additionally, natural products are challenging to standardize and control, which does not lend itself well to modern medical research schemes.
n
[JAMES TAYLOR SEGMENT]
n
We have also covered the fact that Cannabis has an extraordinarily long track record with humans, going back nearly 5000 years or more. Through that time, records of varying degrees of quality have been kept about the medical use and toxicity of Cannabis for thousands of years. The historical record indicates that Cannabis has been considered a potent medicine all the way up until the 1930s when Cannabis prohibition began. We haven’t even discussed the history of Cannabis prohibition here but let me just say – Cannabis prohibition was not backed by science, and many medical associations were unhappy when access to Cannabis was prohibited.
n
Modern research has confirmed that, in fact, many of the traditional medical uses of Cannabis are well-founded and, compared to many foods and drugs, Cannabis is very safe. Where we lack clinical research, we have a host of anecdotal reports, case studies, and observational studies documenting the medical efficacy of Cannabis. And while these types of research may be considered lower quality, at a point these reports become overwhelming in their results. And yet, today in 2019 in the United States, people are still struggling to get legal access to medical Cannabis.
n
While many of you may already be familiar with a little girl named Charlotte Figgi[19] that brought nationwide attention to the treatment of CBD-rich Cannabis for seizures in a famous CNN special with Dr. Sanjay Gupta called Weed[20], you may be less familiar with another little girl that is fighting the same fight in my home state of Mississippi, and her name is Harper Grace[21]. Harper Grace is a little girl that also suffers from seizures, similar to Charlotte. Her parents found that CBD-rich Cannabis was an effective treatment. In 2014, after a lot of advocacy from Harper Grace’s parents and friends, the state legalized CBD oil, in a limited capacity for limited conditions in a limited selection of patients. Since the law passed, which is actually named after Harper Grace, that little girl still has not been able to get access to CBD treatment, and now her parents are fighting for statewide medical marijuana legalization for 2020.
n
[NEWS CLIP]
n
This issue is especially poignant considering the countries only federally sanctioned Cannabis research and development laboratory is located at the University of Mississippi.
nLet’s review what we’ve learned.
n
-
- n
-
- Cannabis has been used as a medicine for a lot of different medical conditions for thousands of years.[22] Up until the early 1940s, Cannabis was even part of the US Pharmacopoeia until prohibition began.
n
-
- Medical research comes in a lot of forms, and we have to be careful not to conflate the statistical significance of an effect measured in a research study with the clinical significance of an effect measured in a therapeutic setting.
n
-
- We can’t assume anything based on a single research result. Research findings always need to be replicated by a different group of researchers.
n
n
-
- There are case studies and uncontrolled clinical research that indicate that Cannabis could be useful for a number of other conditions like autism, ADHD, PTSD, anxiety, depression, and immune system related disorders. While there are numerous case studies and observational reports documenting Cannabis’ efficacy treating conditions like these in patients, it is difficult to interpret that data and extrapolate it to a much larger population.
n
-
- There’s a lot we don’t know. Cannabis comes in a lot of different forms. There are many different chemical profiles of Cannabis, each with its own therapeutic index. We are just scratching the surface with understanding Cannabis and we have a long way to go.
n
-
- We do know that Cannabis is very safe when consumed responsibly. It is impossible to lethally overdose on Cannabis and many of the adverse health risks of Cannabis can be minimized by utilizing oral forms of Cannabis at low dosages. For more information about the safety of Cannabis, check out episodes 1-3 where we explore this topic at length.
n
-
- Clinicians working with patients using Cannabis are seeing positive effects, in general, and at times even profound results. But it’s not a silver bullet. It’s not a cure all. It’s not for every person or every condition. But it is a tool in the clinical tool chest that some people respond very positively to.
n
n
So, how is Cannabis a medicine?
n
Well, simply put, a lot of ways. There is still a lot we don’t know, but there is a lot we do know regarding the safety of Cannabis and the use of Cannabis traditionally as a medicine for thousands of years throughout human history. While, yes, some of the claims about cannabis as a medicine are over-hyped, a lot of them aren’t. A lot of people are finding relief from very serious conditions that they are having to live with every day through the help of Cannabis.
n
Today it seems like the rationale for restricting access to Cannabis or Cannabis products often comes down to an argument around safety and a lack of research. Harper Grace is fighting for access to CBD oil because lawmakers in Mississippi feel that Cannabis needs to be studied more to understand its risks. The FDA has stated that they are unlikely to allow CBD in foods because they want to better understand the potential risks.[25] This issue with CBD safety is particularly interesting considering the World Health Organization already issued a report in 2018 claiming “CBD is generally well tolerated with a good safety profile…To date there is no evidence of any public health-related problems associated with the use of pure CBD.”[26] Despite this determination, the FDA backs their stance by citing a recent rodent study that claimed to have identified the liver damaging effects of CBD[27] – however as we covered in episode one of the podcast – this study was a rodent study that utilized massive, unrealistic, doses of CBD before uncovering damaging effects. At doses more typical of what anyone might encounter in real life – these liver damage effects were not observed.
n
Very recently, democratic presidential candidate and former vice president Joe Biden stated that he believed that there needed to be more research into the risks of Cannabis, particularly as a gateway drug, before legalizing the plant federally.[28] Yet, as we also covered in episode one of the podcast, an administrative law judge in the US in 1988 made a formal statement attesting to the safety profile of Cannabis and the need to reschedule it to a more lenient drug schedule.[29]
n
So, what do you think?
n
Do we need more research into the safety of Cannabis before we legalize nationwide? How much evidence is enough before people are allowed open, legal access to Cannabis for medical purposes around the world?
n
Personally, I was left with a couple of questions:
n
-
- n
-
- Why are Cannabis and its cannabinoids still schedule I drugs in the United States? It’s clear Cannabis has therapeutic applications in certain contexts. Sure, Cannabis can be abused, but so can many other things which are totally legal. Many lawmakers claim we need more research, but how will that research ever take place if Cannabis remains schedule I? Ultimately, the legal status of Cannabis seems to be hurting people more than the plant itself could ever do.
n
-
- Given the safety profile of Cannabis, and its potential efficacy, contrasted with the sometimes-harsh effects of some other medications, why is Cannabis often used as a last resort treatment option for patients, rather than one of the early options?
n
-
- How much of the benefit that users claim they are getting from Cannabis is actually related to its therapeutic activity, and how much might be placebo? And if some of Cannabis’ therapeutic effects are placebo effects – does that matter, if people are finding relief and the treatment is relatively benign?
n
n
So far, we have been looking at the various ways Cannabis is used as a medicine. But what do cannabinoids and other chemicals in Cannabis actually do in the body to elicit these medicinal effects?
n
Join me in our next episode as we take our fantastic voyage into the human body to understand how Cannabis works. In the next episode we begin to explore the question, “What is the endocannabinoid system?”
n
Until next time, I’m your host, Jason Wilson. Thanks, and take it easy.
n
[OUTRO MUSIC]
n
CITATIONS
n
[1] https://www.coloradopotguide.com/images/blog/Health-Effects-of-Marijuana-Reduced.png
{kind=link}
n
[2] https://miro.medium.com/max/1400/0*T-fJXuEjKW4qGUXM.jpg
{kind=link}
n
[3] Rohrig et al. Types of Study in Medical Research. Part 3 of a Series on Evaluation of Scientific Publications. Dtsch Artztebl Int. 2009. 106(15): 262-268.
n
[4] Kabisch et al. Randomized Controlled Trials. Part 17 of a Series on Evaluation of Scientific Publications. Dtsch Artztebl Intl. 2011. 108(39): 663-668.
n
[5] Devlin RB et al. In vitro studies: what is their role in toxicology? Exp Toxicol Pathol. 2005. 57 Supple 1:183-188.
n
[6] Lorian V. Differences between in vitro and in vivo studies. Antimicrob Agents Chemother. 1988. 32(10): 1600-1601.
n
[7] Ghallab A. In vitro test systems and their limitations. EXCLI J. 2013. 12: 1024-1026.
n
[8] Geraghty RJ et al. Guidelines for the use of cell lines in biomedical research. 2014. Br J Cancer. 111(6):1021-1046.
n
[9] Waterbor JW et al. Considerations of sample size in medical research. JAAPA. 2008. 21(4)
n
[10] Mullane K et al. Chapter 1 – Reproducibility in Biomedical Research. Research in the Biomedical Sciences. Transparent and Reproducible. 2018. pp. 1-66.
n
[11] LeFort SM. The Statistical versus Clinical Significance Debate. 1993. 25(1):57-62.
n
[12] Singal AG et al. A Primer on Effectiveness and Efficacy Trials. Clin Transl Gastroenterol. 2014. 5(1): e45.
n
[13] https://www.fda.gov/drugs/development-approval-process-drugs
n
[14] https://www.gwpharm.com/healthcare-professionals/sativex
n
[15] https://www.fda.gov/news-events/press-announcements/fda-approves-first-drug-comprised-active-ingredient-derived-marijuana-treat-rare-severe-forms
n
n
[17] https://www.ama-assn.org/delivering-care/public-health/how-are-prescription-drug-prices-determined
n
[18] Fassbender M. Clinical trial cost is a fraction of the drug development bill, with an average price tag of $19m. 2018. https://www.outsourcing-pharma.com/Article/2018/09/26/Clinical-trial-cost-is-a-fraction-of-the-drug-development-bill
n
[19] https://www.cnn.com/2013/08/07/health/charlotte-child-medical-marijuana/index.html
n
[20] https://www.cnn.com/2013/08/08/health/gupta-changed-mind-marijuana/index.html
n
[21] Rowell N. Harper Grace’s Legacy. North Side Sun. 2019 Apr 11. https://www.northsidesun.com/news-breaking-news/harper-grace%E2%80%99s-legacy
n
[22] Russo E. The Pharmacological History of Cannabis. Chapter 2. Handbook of Cannabis. Oxford University Press. 2014. p.23-29
n
[23] Whiting PF et al. Cannabinoids for Medical Use. A Systematic Review and Meta-Analysis. JAMA. 2015. 313(24): 2456-2473.
n
[24] Hill KP. Medical Use of Cannabis in 2019. JAMA. 2019. 322(10): 974-975.
n
[25] https://www.fda.gov/consumers/consumer-updates/what-you-need-know-and-what-were-working-find-out-about-products-containing-cannabis-or-cannabis
n
[26] World Health Organization (WHO). Cannabidiol (CBD) Critical Review Report. Expert Committee on Drug Dependence. Fortieth Meeting. 2018. https://www.who.int/medicines/access/controlled-substances/CannabidiolCriticalReview.pdf
n
[27] Ewing et al. Hepatotoxicity of a Cannabidiol-Rich Cannabis Extract in the Mouse Model. Molecules. 2019. 24(9): 1694.
n
[28] https://www.washingtonpost.com/nation/2019/11/18/joe-biden-marijuana-gateway-drug-legalization/
n
[29] https://www.nytimes.com/1988/09/07/us/judge-urges-allowing-medicinal-use-of-marijauna.html
n
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
#04 How is Cannabis a Medicine? – Part One: Ancient History to Modern Medicine
Episode Description: In this episode, we begin exploring the idea of Cannabis as a medicine. How has Cannabis been used as a medicine in the past? How is Cannabis being used as a medicine today? What does modern medical research have to say regarding what Cannabis can and can’t treat? Featured guests include Ethan Russo MD, Jason Miller DACM, James Taylor MD, and Kevin Spelman PhD.
Transcript:
You’re listening to the Curious About Cannabis podcast
Before we get started let me share a little disclaimer here. In this episode we are going to be discussing the medical uses of Cannabis. All of the information I present to you in this podcast is for education and entertainment purposes only and should not be considered medical advice. Never make decisions about your health based on anything you hear me or any other podcast host talk about. I’m simply sharing information that I’ve collected from talking with professionals with relevant experience or from research studies that are available. But I’m not a doctor, and you should always get your medical advice from a licensed health care professional. Now with that out of the way, let’s move on.
n
[Shutter]
n
[KEVIN SPELMAN CLIP]
n
Here in the state of Oregon, medical Cannabis has been available since 1998 for registered patients with a doctor’s recommendation. There are a variety of conditions that can qualify someone to join the Oregon Medical Marijuana Program, such as cancer, glaucoma, PTSD, or HIV, but the most common condition being treated with medical Cannabis, by far, is pain. At the time of this recording, in 2019, 88% of the 27,000 qualifying patients in Oregon’s Medical Marijuana Program reported severe pain as a condition that they intended to treat with Cannabis.[1] The remaining conditions ranked from most common to least common are spasms, PTSD, nausea, cancer, neurological disease, seizures, glaucoma, wasting syndrome, HIV/AIDS.[2]
n
Clearly people are trying to treat a wide variety of serious conditions with Cannabis. If Cannabis is an effective therapy for just some or all of these conditions, it could change the health and wellbeing for a massive amount of people currently suffering every day.
n
So what do we really know about Cannabis? How is Cannabis a medicine?
n
[INTRO]
n
Hey everybody, I’m Jason Wilson and you’re listening to the Curious About Cannabis podcast. Thanks for tuning in once again. In this episode we’ll be exploring the idea of Cannabis as a medicine.
n
And to guide our curious quest I wanted to explore several primary questions:
n
-
- n
-
- How has Cannabis been used as a medicine in the past?
n
-
- How are Cannabis and Cannabis derived drugs being used as medicine today?
n
-
- How are medical claims derived? How do we determine that something is a medicine?
n
n
Let’s get started.
n
In 2015 the Journal of the American Medical Association published a review, acknowledging a list of therapeutic applications of Cannabis, while also expressing skepticism over others.[3] The National Academy of the Sciences, Engineering and Medicine released a lengthy 400+ page review also identifying clear therapeutic applications of Cannabis and its constituents.[4]
n
[NEWS CLIP][5]
n
I have to point out here that when we talk about the medical use of Cannabis, we aren’t just talking about smoking Cannabis. There are lots of ways to consume Cannabis, and each consumption method affects the body differently. Sure, Cannabis can be smoked or vaporized, but it can also be eaten in the form of Cannabis infused foods or taken sublingually by taking drops of a Cannabis tincture under the tongue. Cannabis can also be administered on the skin, topically. Less commonly, Cannabis can also be taken as a suppository.
n
Anything consumed orally will take longer to take effect because it has to pass through the digestive system and undergo a process called first-pass metabolism before the cannabinoids are passed into the bloodstream. During this metabolic process, cannabinoids are chemically altered. For instance, when THC is ingested orally, nearly half of the THC is metabolized to a compound called 11-OH-THC, which is considered nearly four times as strong as THC.[6] This is why the experience of eating Cannabis products can be so unique and sometimes more powerful than consuming Cannabis by other means.
n
However, when smoking, vaping, using sublingual products, or suppositories, cannabinoids bypass the liver and pass straight into the blood, leading to a much faster onset and avoiding the chemical alteration that happens during metabolism.
n
So it seems among the scientific and medical communities, there is no doubt that in some contexts, Cannabis can be a medicine. But to what extent? For what conditions? At what dosages? In what form? That is where much of the debate currently resides.
n
According to the United States government, at the time of this recording in 2019, Cannabis and it’s cannabinoid constituents are classified as schedule I drugs, a classification reserved for drugs that are presumed to have no medical value and a high propensity for abuse.[7] Other drugs that are classified as schedule I include things like heroin and bath salts. To put this into perspective, drugs like cocaine and methamphetamine, which are schedule II drugs, are less controlled than Cannabis.
n
Despite the US government’s determination that Cannabis should be a schedule I drug and as such has no medical value – the government actually held a patent on the antioxidant and neuroprotective properties of cannabinoids up until this year.[8] To many, this patent represented deep hypocrisy.
n
Regardless of the legal status of Cannabis, there are many people across the US that have jumped on the Cannabis bandwagon, touting benefits so profound and diverse that it can’t help but sound like a pitch for the next snake oil.
n
[JASON MILLER]
n
That’s Dr. Jason Miller, a medicinal plant and Chinese medicine expert that has been noticing that more and more of his patients are talking about Cannabis.
n
[JASON MILLER]
n
So what’s the truth here? To start, let’s explore the ways Cannabis has been used as a medicine throughout history. Then we can look at some of the more modern Cannabis research and see how some of these traditional uses hold up against modern science.
n
n
How has Cannabis been used as a medicine in the past?
n
Cannabis has been used by humans for a long, long, long time. We’re talking thousands of years. We’re talking 5000 years. Half of a decamillenium. Decamillenium? Is that a word? It is now.
n
[JASON MILLER]
n
In Chapter 2 of the book the Handbook of Cannabis, Ethan Russo, a neurologist and cannabinoid researchers that has been studying Cannabis for over 25 years, summarizes some of the ways in which Cannabis was used therapeutically throughout the last several millenia.[9] Here’s an extremely condensed version.
n
Oral traditions of Cannabis use for appetite stimulation and fighting the effects of old age date back to nearly 3000 years BCE.[10] That’s 5000 years ago! In 1500 BCE, the Atharva Veda indicates that Indians were using Cannabis for anxiety relief.[11] Cannabis is suspected to even be a component of the holy anointing oil of the Hebrews as far back as 750 BCE.[12] [13] The juice of the leaves was noted to be a remedy for earaches in the first century.[14] In the second century Chinese records indicate Cannabis was used in wine as an anesthetic.[15] In the early 10th century Persian records indicate it was even used to stimulate hair growth.[16] In 1542 it was noted that the Cannabis roots could be boiled and used to treat gout and burns.[17] Throughout the 16th century records indicate Cannabis was used for sore muscles, stiff joints, burns, wounds, jaundice, colic and even tumors.[18]
n
In 1839 a researcher named O’Shaughnessy studied Indian use of Cannabis and performed experiments in dogs, and then later people, to determine if Cannabis was a suitable treatment for tetanus, rabies, epilepsy and rheumatoid disease.[19] Shortly after O’Shaughnessy published his findings, Cannabis began showing up in the European and United States Pharmacopoeias.
n
O’Shaughnessy is a particularly interesting figure in the history of medical Cannabis. We are going to be learning more about his work in future episodes.
n
As records become more easily obtainable, we can find records throughout the 18th and 19th centuries of Cannabis being used to treat migraines, pain, spasticity, anxiety, depression, and insomnia.[20]
n
Cannabis was even featured in the US Pharmacopoeia as a medicine until the 12th edition released in 1942 after marijuana prohibition had begun in 1937.[21] You can still look up old issues of the USP and look for Extractum Cannabis or Tinctura Cannabis aka Extract of Hemp or Tincture of Hemp. Upon the initial publication of Cannabis in the USP in 1851, the 9th edition of the US Dispensatory had this to say about the medical use of Cannabis: “It has been found to cause sleep, to allay spasm, to compose nervous disquietude, and to relieve pain…The complaints in which it has been specially recommended are neuralgia, gout, rheumatism, tetanus, hydrophobia, epidemic cholera, convulsions, chorea, mental depression delirium tremens, insanity, and uterine hemorrhage.”[22]
n
After Cannabis prohibition began, Cannabis became unavailable as a medicine, and research into the plant progressively slowed down into the late 1950s. Modern medical research into Cannabis really took off in the 1960s when THC was isolated and synthesized.[23] A little known fact – but CBD was actually isolated and characterized approximately 20 years prior to when THC was isolated.[24] But because CBD did not elicit an intoxicating effect, it was largely ignored at first.
n
As THC research progressed throughout the 1960s and 1970s, research confirmed that THC could reduce nausea and vomiting associated with cancer chemotherapy[25], that THC had the same analgesic activity as codeine[26], and that THC performed as well as the anti-asthma drug salbutamol aka albuterol or Ventolin as a bronchodilator.[27]
n
The 1980s ushered in renewed interest in CBD as well as continued research on THC. In 1981 CBD was identified as an anticonvulsant.[28] A year later it would be found that CBD could help relieve the anxiety brought on by THC.[29] In 1985, the unique flavonoid Cannflavin A was discovered, breaking Cannabis research away from the cannabinoid chemical class to encompass other types of plant compounds.[30] It was also in 1985 that the pharmaceutical drug Marinol was approved by the FDA for chemotherapy related nausea.[31]
n
[ETHAN RUSSO]
n
That’s Ethan Russo, and he knows a thing or two about cannabinoid pharmaceuticals.
n
[ETHAN RUSSO]
n
And then in 1988 scientists finally discovered a chemical receptor in the body that seemed to be responsible for most of THC’s effects – the cannabinoid type 1 receptor, or CB1 receptor.[32] This marks the beginning of piecing together a fascinating puzzle about a physiological system that had since been ignored – the endocannabinoid system, which wouldn’t be formally named for another 10 years.[33] But we’ll get into that story in another episode.
n
In 1993 CBD’s anti-anxiety effects that had been previously noted in the 1980s was again confirmed.[34]
n
In 1997 it was found that THC could help reduce agitation in patients with dementia.[35]
n
In 2003 clinical trials of the Cannabis based pharmaceutical Sativex began, investigating whether it could be effective in treating multiple sclerosis symptoms.[36] In 2005 Sativex would go on to be approved in Canada for the treatment of MS related pain.[37] Over the years Sativex would later be approved for other types of pain such as neuropathic pain and cancer pain.[38] [39] Eventually Sativex would be approved in the UK and Spain for spasticity in MS patients.[40] In 2010 it would be discovered that Sativex can also treat nausea related to chemotherapy treatments.[41]
n
[ETHAN RUSSO]
n
Over and over, health care professionals I spoke with commented on the superior efficacy of broader spectrum Cannabis products over isolated cannabinoids.[42]
n
[JAMES TAYLOR]
n
This is Dr. James Taylor, a pain physician working in North Carolina. Ever since hemp became federally legal in the United States, he has been working with his patients to understand how hemp extracts, and CBD particularly, might be a tool to help treat chronic pain.
n
[JAMES TAYLOR]
n
This difference in therapeutic outcome between isolated compounds from Cannabis and the use of herbal Cannabis or broad-spectrum Cannabis extracts is attributed to something often called – the entourage effect.[43]
n
[KEVIN SPELMAN]
n
So far we have looked at the ways in which Cannabis has been used as a medicine in the past, and some ways in which Cannabis and cannabinoid drugs are being used as medicine today. Join us in part two of this series where we pick up on our quest to understand Cannabis as a medicine by examining the ways in which medical claims are derived. How do we determine that something is a medicine? And what results are clinicians seeing in their patients that are using Cannabis?
n
Until next time, I’m your host, Jason Wilson, stay curious and take it easy!
n
n
n
[1] Oregon Medical Marijuana Program Statistical Snapshot October 2019. https://www.oregon.gov/oha/PH/DISEASESCONDITIONS/CHRONICDISEASE/MEDICALMARIJUANAPROGRAM/Documents/OMMP_Statistical_Snapshot_10-2019.pdf
n
[2] Oregon Medical Marijuana Program Statistical Snapshot October 2019. https://www.oregon.gov/oha/PH/DISEASESCONDITIONS/CHRONICDISEASE/MEDICALMARIJUANAPROGRAM/Documents/OMMP_Statistical_Snapshot_10-2019.pdf
n
[3] Whiting PF, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. 2015. 313(24): 2456-2473.
n
[4] National Academies of Sciences, Engineering, and Medicine. 2017. The health effects of cannabis and cannabinoids: Current state of evidence and recommendations for research. Washington, DC: The National Academies Press.
n
[5] CBS This Morning. New Report Finds Benefits and Risks of Marijuana. https://www.youtube.com/watch?v=Jx6ioVF5KhE&t=13s
n
[6] Huestis MA. Human Cannabinoid Pharmacokinetics. Chem Biodivers. 2007. 4(8): 1770-1804.
n
[7] Lists of Scheduling Actions Controlled Substances and Regulated Chemicals. United States Department of Justice. Drug Enforcement Administration. https://www.deadiversion.usdoj.gov/schedules/orangebook/orangebook.pdf
n
[8] Hampson et al. Cannabinoids as antioxidants and neuroprotectants. Patent US6630507B1. https://patents.google.com/patent/US6630507B1/en
n
[9] Russo E. The Pharmacological History of Cannabis. Chapter 2. Handbook of Cannabis. Oxford University Press. 2014. p.23-29
n
[10] Shou-Zhong, Y. The Divine Farmer’s Materia Medica: A Translation of the Shen Nong Ben Cao Jing. 1997. Boulder, CO: Blue Poppy Press.
n
[11] Grierson, GA. The hemp plant in Sanskrit and Hindi literature. Indian Antiquary. 1894. 260-262.
n
[12] Alter R. The Five Books of Moses: A Translation with Commentary. 2004. New York: W.W. Norton & Co.
n
[13] Russo EB. History of Cannabis and its preparations in saga, science and sobriquet. Chemistry and Biodiversity. 2007. 4: 2624-2648.
n
[14] Dioscorides P and Beck LY. De Materia Medica. 2011. Hildesheim: Olms-Weidmann.
n
[15] Julien MS. Chirugie chinoise. Substance anesthétique employée en Chine, dans le commencement du III-ième siecle de notre ère, pour paralyser momentanement la sensibilité. Comptes Rendus
n
Hebdomadaires de l’Académie des Sciences. 1849. 28:223–229.
n
[16] Lozano I. The therapeutic use of Cannabis sativa L. in Arabic medicine. Journal of Cannabis Therapeutics. 2001. 1: 63-70.
n
[17] Fuchs L. The great herbal of Leonhart Fuchs: De historia stirpium commentarii insignes, 1542 (notable commentaries on the history of plants). 1999. Stanford, CA: Stanford University Press.
n
[18] Gerard J and Johnson T. The Herbal: or, General History of Plants. 1975. New York: Dover Publications
n
[19] O’Shaughnessy WB. (1838–1840). On the preparations of the Indian hemp, or gunjah (Cannabis indica); their effects on the animal system in health, and their utility in the treatment of tetanus and other convulsive diseases. Transactions of the Medical and Physical Society of Bengal, 71–102, 421–461.
n
[20] Russo E. The Pharmacological History of Cannabis. Chapter 2. Handbook of Cannabis. Oxford University Press. 2014. p.23-29
n
[21] United States Pharmacopoeia 12th Edition. 1942
n
[22] George B. Wood and Franklin Bache, eds., 1851, The Dispensatory of the United States of America, 9th ed. Philadelphia: Lippincott, Grambo, 1851, pp. 310-311.
n
[23] Gaoni Y and Mechoulam R. Isolation, Structure, and Partial Synthesis of an Active Constituent of Hashish. J. Am. Chem. Soc. 1964. 86(8): 1646-1647.
n
[24] Adams R et al. Structure of Cannabidiol, a Product Isolated from the Marihuana Extract of Minnesota Wild Hemp. I. J. Am. Chem. Soc. 1940. 62(1): 196-200.
n
[25] Sallan SE et al. Antiemetic effect of delta-9-tetrahydrocannabinol in patients receiving cancer chemotherapy. New England Journal of Medicine. 1975. 293: 795–797.
n
[26] Noyes R Jr et al. The analgesic properties of delta-9- tetrahydrocannabinol and codeine. Clinical Pharmacology and Therapeutics. 1975. 18: 84–89.
n
[27] Williams, SJ et al. Bronchodilator effect of delta1-tetrahydrocannabinol administered by aerosol of asthmatic patients. Thorax. 1976. 31: 720–723.
n
[28] Carlini EA and Cunha JM. Hypnotic and antiepileptic effects of cannabidiol. Journal of Clinical Pharmacology. 1981. 21: 417S–427S.
n
[29] Zuardi AW et al. Action of cannabidiol on the anxiety and other effects produced by delta 9-THC in normal subjects. Psychopharmacology. 1982. 76: 245–250.
n
[30] Barrett ML et al. Isolation from Cannabis sativa L. of cannflavin – a novel inhibitor of prostaglandin production. Biochemical Pharmacology. 1985. 34: 2019–2024.
n
[31] Russo E. The Pharmacological History of Cannabis. Chapter 2. Handbook of Cannabis. Oxford University Press. 2014. p.23-29
n
[32] Devane WA et al. Determination and characterization of a cannabinoid receptor in rat brain. Molecular Pharmacology. 1988. 34: 605–613.
n
[33] Di Marzo V. ‘Endocannabinoids’ and other fatty acid derivatives with cannabimimetic properties: biochemistry and possible physiopathological relevance. Biochimica et Biophysica Acta. 1998. 1392: 153–175
n
[34] Zuardi AW et al. Effects of ipsapirone and cannabidiol on human experimental anxiety. Journal of Psychopharmacology. 1993. 7: 82–88.
n
[35] Volicer, L et al. Effects of dronabinol on anorexia and disturbed behavior in patients with Alzheimer’s disease. International Journal of Geriatric Psychiatry. 1997. 12: 913–919.
n
[36] Wade, DT et al. A preliminary controlled study to determine whether whole-plant cannabis extracts can improve intractable neurogenic symptoms. Clinical Rehabilitation. 2003. 17: 18–26.
n
[37] Rog DJ et al. Randomized controlled trial of cannabis based medicine in central neuropathic pain due to multiple sclerosis. Neurology. 2005. 65: 812–819.
n
[38] Notcutt W et al. Initial experiences with medicinal extracts of cannabis for chronic pain: results from 34 “N of 1” studies. Anaesthesia. 2004. 59: 440–452.
n
[39] Berman JS et al. Efficacy of two cannabis based medicinal extracts for relief of central neuropathic pain from brachial plexus avulsion: results of a randomised controlled trial. Pain. 2004. 112: 299–306.
n
[40] Novotna A et al. A randomized, double-blind, placebo-controlled, parallel group, enriched-design study of nabiximols (Sativex®), as add-on therapy, in subjects with refractory spasticity caused by multiple sclerosis. European Journal of Neurology. 2011. 18: 1122–1131.
n
[41] Duran M et al. Preliminary efficacy and safety of an oromucosal standardized cannabis extract in chemotherapy-induced nausea and vomiting. British Journal of Clinical Pharmacology. 2010. 70: 656–663.
n
[42] Russo EB. The case for the entourage effect and conventional breeding of clinical cannabis: no “strain,” no gain. Front. Plant Sci. 09 January 2019. https://doi.org/10.3389/fpls.2018.01969
n
[43] Ben-Shabat S et al. An entourage effect: inactive endogenous fatty acid glycerol esters enhance 2-arachidonoyl-glycerol cannabinoid activity. European Journal of Pharmacology. 1998. 353: 23–31.
n
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
BTS #02: Matt Vogel on Drug Education, Adolescent Cannabis Use, Harm Reduction and Health
In this behind-the-scenes full length interview, I speak with health and wellness educator Matt Vogel at length (over 2 hours) about drug education in the United States, issues surrounding adolescent Cannabis use, harm reduction strategies to minimize the risks of drug use, the problem of confirmation bias when researching Cannabis, and much more! This was actually the very first interview for the podcast, so it might present itself a bit differently than other interviews for this season.
Learn more about the Curious About Cannabis Podcast by visiting www.CACPodcast.com
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
#03 Is Cannabis Safe? Part Three: Adolescent Use and Harm Reduction
Episode Description: In this episode of the Curious About Cannabis Podcast we wrap up our three-part series on Cannabis safety and harm reduction by exploring the question, “Is Cannabis Safe?”. First we talk about adolescent Cannabis use before discussing ways in which Cannabis users can minimize or eliminate many of the risks associated with Cannabis. Make sure you listen to episodes 1 and 2 prior to listening to this episode!
Episode Transcript:
#03 Is Cannabis Safe? Part Three: Adolescent Cannabis Use and Harm Reduction
You’re listening to the Curious About Cannabis Podcast.
[Reefer Madness Clip]
[Shutter]
Hey everybody, this is Jason Wilson with the Curious About Cannabis podcast, thanks so much for tuning in once again. Over the last two episodes we have been exploring the topic of Cannabis safety and harm reduction. We explored the toxicity of some of the major chemical constituents of Cannabis resins, how Cannabis can interact with medications, and contaminants that could be found in Cannabis products. Now, for this third and final part of this series, we are focusing on the topics of teen Cannabis use before diving into some of the ways that Cannabis users can minimize the potential risks associated with Cannabis use.
n
So here we go, the third and final part of our series where we explore the question: “Is Cannabis Safe?”
n
[INTRO MUSIC]
n
What about adolescent Cannabis use?
n
What are the risks of exposing children to Cannabis at an early age? As you might imagine, this is a very complicated question. For this episode we are going to ignore the topics of Cannabis use during pregnancy, while breastfeeding, or medical Cannabis use in children. We’ll explore those topics in other episodes. For this episode, we are going to focus on looking at the health risks of adolescent Cannabis use during the teenage years.
n
The topic of adolescent Cannabis use is a complicated and sensitive topic. Kids today have become very wary of drug education of any kind, primarily because kids have been exposed to tales of exaggerated harms or outright lies about drug use for decades as part of prohibition and abstinence-based drug education programs.[1] [2]
n
[MATT VOGEL SEGMENT]
n
This is Matt Vogel. Matt is a health and wellness educator that works with high school and college students to teach about health, substance use, and harm reduction strategies.
n
[MATT VOGEL SEGMENT]
n
Regarding Cannabis, kids have been told that it will kill brain cells, lead to schizophrenia or other mental health issues, make them lazy or stupid, or cause them to move on to other drugs like cocaine or heroin.
n
It should first be pointed out that there are big differences between acute or occasional Cannabis use and chronic Cannabis use. In general, acute Cannabis use is pretty safe, physiologically, with the biggest risks being risks of motor discoordination, which is why it is not a good idea to drive after using THC-rich Cannabis, memory disruption, and psychological distress.[3] However, most of the major risks that adolescents learn about Cannabis are associated with chronic, or repeated, Cannabis use.
n
While chronic Cannabis use can alter the way the brain functions[4] [5] [6], and we need to understand the consequences of that more, to say that it kills brain cells is dishonest. Cannabis can make some parts of the brain less active while making other parts of the brain more active.[7] In fact, in some cases Cannabis can actually encourage new brain cells to grow in a process called neurogenesis[8] [9].
n
While Cannabis can exacerbate or reveal underlying mental health problems in adolescents, there is not strong evidence that it actually causes these problems.[10] [11] And the only time that Cannabis seems to act as a gateway to other drugs seems to be when users are exposed to those other drugs on the black market.[12]
n
The issue of adolescent Cannabis use and IQ is a more complicated problem. Research has confirmed that there does not seem to be a link between Cannabis use and low IQ, but there does seem to be a link between early onset Cannabis use and poor cognitive performance.[13] [14] If you dig through the research, a common theme emerges. The issue is that THC in Cannabis can, in some people, interfere with the learning process, by disrupting attention and memory. Ultimately users that are affected in this way have to work harder to perform as well as they typically would without Cannabis.
n
Depending on the situation, Cannabis use can also cause kids to avoid social interactions, which can cause problems with the development of emotional intelligence and social skills.[15] [16] [17] Chronic THC-rich Cannabis use can interfere with learning processes at a time when a person is going through critical developmental stages, resulting in poor development into adulthood. Although the brain is not actually a muscle, it acts like one in the sense that if you don’t exercise it, it won’t perform well.
n
But a lot of these possible outcomes are difficult to assess[18] because there are a lot of variables that affect a person’s cognitive development including social factors, concurrent drug use, such as alcohol use, and underlying mental health disorders to name a few. In addition, everyone responds to Cannabis differently. There are also a wide variety of Cannabis products, with different risks associated with them.
n
It has to be noted here, that the context of Cannabis use has a lot to do with outcomes. There are children, teens, and adults throughout the world with qualifying medical conditions that are using Cannabis medically and exhibiting very few adverse events.[19] [20] In addition, CBD rich Cannabis or Cannabis products that don’t have intoxicating effects do not present the same psychological health risks as THC rich Cannabis products. Dose is also an important factor to consider. Lower dosages of either THC or CBD present fewer risks than higher doses.
n
So if Cannabis can be used responsibly, while minimizing adverse events, then what does that look like?[21] When does Cannabis use become Cannabis abuse?
n
[MATT VOGEL SEGMENT]
n
One thing I really appreciated about my conversation with Matt was his attention to how complicated this topic is, and that there is no one size fits all answer regarding teen Cannabis use and the potential risks involved. Even just finding reputable information about Cannabis can be challenging in the age of internet headlines and memes
n
[MATT VOGEL SEGMENT]
n
So, let’s assume an adolescent has decided that they want to experiment with Cannabis. How long should they wait in order to stay safe?
n
[MATT VOGEL SEGMENT]
n
How can people minimize the risks of using Cannabis?
n
This all begs the next question, what can people do to reduce the risks associated with Cannabis use? From Matt’s perspective, that begins with cultivating a healthy amount of self-awareness regarding not only substance use, but health and wellness in general.
n
[MATT VOGEL SEGMENT]
n
And beyond all of that, Matt had a simple recommendation to reduce risk that was echoed by many of my other guests.
n
[MATT VOGEL SEGMENT]
n
I asked veteran Cannabis and cannabinoid researcher, Dr. Ethan Russo, about his thoughts on minimizing risks associated with Cannabis use. Right away he wanted to bring attention to the diverse and sometimes uncertain quality of Cannabis products on the market.
n
[ETHAN RUSSO SEGMENT]
n
So it’s clear that the first step of minimizing risk is to ensure you find clean, high quality products. But what comes next? Many people understand that it can be a very uncomfortable and unpleasant experience to take too much Cannabis, so what can people do to avoid this?
n
I spoke with Dr. Jason Miller about this issue. Jason is a doctor of acupuncture and Chinese medicine that is an expert regarding the clinical use of medicinal plants. Recently he started having a lot of patients coming to him to ask about Cannabis, so he began taking note of what their experiences and outcomes were like in order to be prepared to counsel others on the potential pitfalls and promises of Cannabis use.
n
The first goal, he noted, was to develop strategies to avoid taking too much in the first place…
n
[JASON MILLER SEGMENT]
n
Okay, so let’s say you’ve done your best to find your minimum effective dose, and you still went too far and are in the midst of an uncomfortable Cannabis experience. What can be done?
n
[JASON MILLER SEGMENT]
n
In case you don’t know, Acetylcholine is a neurotransmitter in our brains that among many things is responsible for influencing things like sleep, arousal, memory, and attention.[22] [23] [24] [25] [26]
n
[JASON MILLER SEGMENT]
n
And if you forget all of these suggestions, there are some products on the market now that claim to combat Cannabis intoxication.
n
[PEGGY ANDERSON SEGMENT]
n
That’s Peggy Anderson, the founder of a company called Canna Help You? Which is dedicated to providing seniors with education about Cannabis. In one recent study, it was found that the demographic of Cannabis users over the age of 65 is growing faster than any other demographic of older adults. Many of these users don’t want to be intoxicated and are particularly concerned about taking too much THC. Peggy shared some of her experience with this issue.
n
[PEGGY ANDERSON SEGMENT]
n
The feedback I got from some of my guests mirrors some of the suggestions found in literature dating back all the way to the 10th century. See Taming THC by Ethan Russo.[27]
n
I asked some of my guests whether they thought that Cannabis products, overall were safe or not. The response was consistent. In places where Cannabis is legal and the quality of Cannabis products are regulated, Cannabis seems to be safer than it has ever been.
n
[ANTHONY SMITH SEGMENT]
n
[PEGGY ANDERSON SEGMENT]
n
Alright, Let’s review what we’ve learned, across these past three episodes:
n
-
- n
-
- While the exact level of toxicity of cannabinoids is unclear, we know that cannabinoids are orders of magnitude less toxic than caffeine or nicotine. It is physically impossible to lethally overdose on herbal As far as extracts and concentrates are concerned – there are a lot of unknowns. There is no long-term safety data available yet to understand how chronic consumption of Cannabis concentrates might affect health, however we do know that a variety of contaminants in Cannabis can become concentrated in Cannabis extracts, presenting greater risk to consumers – particularly those that have pre-existing health problems.
n
-
- Although Cannabis is unlikely to present the risk of a lethal overdose, there are still health risks to users, including risks to lung health, heart health, mouth health, immune system health and mental health.n
-
- n
-
- Many of these health risks stem from smoking and can be minimized or eliminated by using other consumption methods like vaporizing[28] or using edibles, tinctures or sublingual products.
n
-
- Naïve users are at greater risk for experiencing psychological adverse effects than experienced users.[29] Start low, go slow.
n
n
-
- Although Cannabis is unlikely to present the risk of a lethal overdose, there are still health risks to users, including risks to lung health, heart health, mouth health, immune system health and mental health.n
n
-
- Cannabis can potentially interact with other medications.[30] Usually this leads to sedation, but in some cases, particularly with CBD, Cannabis could slow down the body’s ability to metabolize drugs, resulting in elevated concentrations of those drugs in the blood. For anyone taking medications with narrow safety windows, this could be dangerous.
n
-
- Some people with pre-existing health conditions could be at greater risk to suffer adverse events from Cannabis use. If you are using Cannabis and have a heart condition, compromised immune system, diabetes, or mental health condition – it’s best to work with a health care professional to make sure you stay safe.
n
-
- Cannabis use in adolescents can exacerbate underlying mental health issues. In general it is best for young people to wait as long as possible before trying Cannabis, ideally until the age of 25, as this is the age when the brain is thought to have reached maturity.
n
-
- If you decide to use Cannabis, start with a low dose and slowly work your way up. If you end up getting too high, there are a number of home remedies to counteract the effects of THC, including drinking water or warm milk, eating peppercorns or black pepper, taking tinctures of passionflower or calamus root, chewing on pine nuts, or drinking lemonade. There are even some targeted Cannabis antidotes now on the market. In addition, CBD may help curb the effects of THC to some extent.
n
-
- Finally, if you consume Cannabis regularly, it’s important to perform regular abstinence breaks and wellness audits to evaluate your relationship with Cannabis to ensure that your Cannabis use is not negatively impacting your health.
n
n
So, is Cannabis safe? In toxicology it is well known that nearly anything can be toxic when consumed in a particular way or in a particular dose. In the early 1500s, the swiss physician, alchemist, and astrologer Paracelsus said, “All things are poison, and nothing is without poison. It is the dose alone that makes a thinit so a thing is not a poison.”[31] Today this is often simplified to the saying, “The dose makes the poison.” This applies to everything, including the water we drink and the air we breathe. Nothing in life is without risk, but in general Cannabis is safer, physiologically, than many substances we engage everyday, like coffee.
n
While there are some rare exceptions and contraindications to be aware of, Cannabis, as long as it is clean, seems to be pretty safe and well tolerated by most people, especially at low doses. Deaths attributed to Cannabis are extremely rare[32] [33], and most adverse events that could arise from Cannabis use, like hyperemesis syndrome[34], are usually reversible. To minimize risk, wait as long as you can to try Cannabis for the first time, avoid smoking, only use Cannabis of a known quality, start with low dosages, and slowly increase dosage to find a minimum effective dose. And remember, if you do take too much THC and are having an uncomfortable experience, there are a variety of things you can do to help ease that uncomfortable feeling, and, most importantly, the feeling will eventually pass and you will be fine.
n
I know that some of you listening might be wondering about the issue of substance abuse and addiction as a risk, which I did not cover in these episodes. Don’t worry, there will be an episode dedicated to that issue, as well as issues like pediatric Cannabis use and Cannabis use while pregnant or breastfeeding. So stay tuned as we revisit the issue of Cannabis safety in other episodes.
n
And with that, I’m your host, Jason Wilson. Until next time, stay curious.
n
[OUTRO Music]
n
Special thanks to our guests that were so gracious in spending time with me for interviews. To check out the citations for this episode, and there are plenty, you can check out the show notes by visiting CACPodcast.com. If you want to learn more about Cannabis, you can check out the Curious About Cannabis book, available on Amazon.com and other online book retailers. If you like what we are doing and want to support the show please consider supporting the podcast by liking and sharing this episode. You can also support us on Patreon at patreon.com/naturallearningenterprises where you can get access to the full-length guest interviews, behind-the-scenes content, and more! You can also connect with Curious About Cannabis on social media on Instagram, Facebook, Twitter, and YouTube.
n
[OUTRO Music continues]
n
n
Citations:
n
[1] Rosenbaum DP, et al. Cops in the Classroom: A Longitudinal Evaluation of Drug Abuse Resistance Education (DARE). Journal of Research in Crime and Delinquency. 1994. 31(1): 3-31.
n
[2] Birkeland S et al. Good reasons for ignoring good evaluation: the case of the drug abuse resistance education (D.A.R.E.) program. Evaluation and Program Planning. 28(3): 247-256.
n
[3] Karilla L et al. Acute and long-term effects of cannabis use: a review. Curr Pharm Des. 2014. 20(25): 4112-4118
n
[4] Ashtari M et al. Medial temporal structures and memory functions in adolescents with heavy cannabis use. Journal of Psychiatric Research. 2011. 45(8): 1055-1066.
n
[5] Demirakca T et al. Diminished gray matter in the hippocampus of cannabis users: possible protective effects of cannabidiol. Drug and Alcohol Dependence. 114(2-3): 242-245.
n
[6] Steel R et al. Delta-9-tetrahydrocannabinol disrupts hippocampal neuroplasticity and neurogenesis in trained, but not untrained adolescent Sprague-Dawley rats. Brain Research. 2014. 1548: 12-19.
n
[7] Jager G et al. Cannabis use and memory brain function in adolescent boys: a cross-sectional multicenter functional magnetic resonance imaging study. J Am Acad Child Adolesc Psychiatry. 2010. 49(6): 561-572.
n
[8] Wolf SA et al. Cannabinoid receptor CB1 mediates baseline and activity-induced survival of new neurons in adult hippocampal neurogenesis. Cell Communication and Signaling. 2010. 8:12.
n
[9] Jiang W et al. Cannabinoids promote embryonic and adult hippocampus neurogenesis and produce anxiolytic and antidepressant like effects. Neuroscience. 2005. 115(11): 3104-3116.
n
[10] Rubino T et al. Adolescent exposure to cannabis as a risk factor for psychiatric disorders. J Psychopharmacol. 2012. 26(1): 177-188.
n
[11] Johns A. Psychiatric effects of cannabis. Br J Psychiatry. 2001. 178: 116-122.
n
[12] Hall W and Lynskey M. Is cannabis a gateway drug? Testing hypotheses about the relationship between cannabis use and the use of other illicit drugs. Drug and Alcohol Review. 24(1): 39-48
n
[13] Jackson N et al. Impact of adolescent marijuana use on intelligence: Results from two longitudinal twin studies. PNAS. 113(5):E500-E508.
n
[14] Harvey M et al. The relationship between non-acute adolescent cannabis use and cognition. Drug and Alcohol Review. 26(3): 309-319.
n
[15] Nehra DK et al. Emotional intelligence and self esteem in cannabis abusers. Journal of the Indian Academy of Applied Psychology. 38(2): 385-393.
n
[16] Nehra DK et al. Alexithymia and emotional intelligence among people with cannabis dependence and health control: a comparative study. Dysphrenia. 2013. 5(1): 49-55.
n
[17] Limonero JT et al. Perceived emotional intelligence and its relation to tobacco and cannabis use among university students. Psicothema. 2006. 18: 95-100.
n
[18] Pope HG et al. Early-onset cannabis use and cognitive deficits: what is the nature of the association? Drug and Alcohol Dependence. 2003. 69(3):303-310.
n
[19] Sznitman SR and Zolotov Y. Cannabis for therapeutic purposes and public health and safety: a systematic and critical review. International Journal of Drug Policy. 2015. 26(1): 20-29
n
[20] Blake DR et al. Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology. 2005. 45(1): 50-52.
n
[21] Lau N et al. Responsible and controlled use: older cannabis users and harm reduction. International Journal of Drug Policy. 2015. 26(8): 709-718.
n
[22] Acetylcholine. Neuroscience. 2nd Edition. https://www.ncbi.nlm.nih.gov/books/NBK11143/
n
[23] Miyazawa M and Yamafuji C. Inhibition of Acetylcholinesterase Activity by Bicyclic Monoterpenoids. J Agric Food Chem. 2005. 53(5): 1765-1768.
n
[24] Ryan MF and Byrne O. Plant-insect coevolution and inhibition of acetylcholinesterase. Journal of Chemical Ecology. 1988. 14(10): 1965-1975.
n
[25] Pattanaik J et al. Acorus calamus Linn.: A herbal tonic for central nervous system. Journal of Scientific and Innovative Research. 2013. 2(5): 950-954.
n
[26] Mukherjee PK et al. In vitro Acetylcholinesterase inhibitory activity of the essential oil from Acorus calamus and its main constituents. Planta Med. 2007. 73(3): 283-285.
n
[27] Russo EB. Taming THC: potential cannabis synergy and phytocannabinoids-terpenoid entourage effects. Br J Pharmacol. 2011. 163(7): 1344-1364.
n
[28] Abrams D et al. Vaporization as a Smokeless Cannabis Delivery System: A Pilot Study. Clinical Pharmacology and Therapeutics. 82(5): 572-578.
n
[29] Volkow ND et al. Adverse Health Effects of Marijuana Use. N Engl J Med. 2014. 370: 2219-2227.
n
[30] Bornheim LM et al. Characterization of cannabidiol-mediated cytochrome P450 inactivation. Biochemical Pharmacology. 1993. 45(6): 1323-1331.
n
[31] Paracelsus, dritte defensio, 1538.
n
[32] Gargani Y et al. Too Many Mouldy Joints – Marijuana and Chronic Pulmonary Aspergillosis. Mediterr J Hematol Infect Dis. 2011. 3(1): e2011005.
n
[33] Bachs L and Morland H. Acute cardiovascular fatalities following cannabis use. Forensic Science International. 2001. 124(2-3): 200-203.
n
[34] Simonetto DA et al. Cannabinoid Hyperemesis: A Case Series of 98 Patients. Mayo Clinic Proceedings. 87(2): 114-119.
n
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More
#02 Is Cannabis Safe? – Part Two: Contaminants in Cannabis
Episode Description: Continuing from our previous episode, we continue exploring the basic question, “Is Cannabis Safe?”, this time focusing on contaminants that could be found in Cannabis or Cannabis products. We speak with biochemist Dr. Anthony Smith about what contaminants labs are commonly finding in Cannabis. We also speak with herbal scientist, Travis Simpson, about his concerns regarding Cannabis processing operations and the potential contaminants that may be introduced to products through bad manufacturing practices. Finally we talk again with neurologist and cannabinoid researcher, Dr. Ethan Russo, to discuss the “vaping crisis” that has claimed the lives of as many as 37 people in the United States and affected nearly 2000 users. This is part two of a three part series exploring the question, “Is Cannabis Safe?”
Transcript:
You’re listening to the Curious About Cannabis Podcast.
[Intro Preview]
[Shutter]
Hey everybody, this is Jason Wilson with the Curious About Cannabis podcast. Thanks so much for tuning in once again. This episode is part two of a three-part series exploring Cannabis safety and harm reduction. If you haven’t listened to the first part of this series, I really recommend stopping this episode and going back to listen to this series from the beginning.
Previously we explored some of the main chemicals in Cannabis, the adverse health risks associated with Cannabis, and how Cannabis can interact with medications.[1] Today we will be focusing on a critical topic that has a huge impact on the safety of Cannabis products – Cannabis contaminants.
n
[INTRO MUSIC]
n
What contaminants might be found in Cannabis products?
n
Anthony Smith is a biochemist that has spent that last five years analyzing Cannabis products for potency and purity in labs all across the United States and Canada.
n
[ANTHONY INTERVIEW SEGMENT]
n
Before we continue, let’s talk a little more about pesticides. Many pesticides are designed to disrupt the nervous systems or hormone signaling in insects.[2] The problem is that this same effect can happen in humans, if someone is exposed to enough of a certain pesticide for long enough periods of time.[3] Additionally, some pesticides, like myclobutanil, a common fungicide[4], can degrade into toxic compounds like hydrogen cyanide when heated.[5]
n
You might be thinking, what’s the big deal about pesticides in Cannabis? Aren’t we already exposed to pesticides through our food? Well, that’s true, but the problem relates to the way in which Cannabis is consumed. When you eat something, your body works hard to ensure that any toxins are captured, broken down, and excreted from the body before they have a chance to reach your blood stream.[6] But when you smoke something, you are bypassing those metabolic processes, and the compounds that enter the lung will pass directly into the blood stream.[7] So essentially when you smoke you are bypassing your body’s natural defense systems that might otherwise keep you safer.
n
It’s also really important to point out that many pesticides, as well as mycotoxins, can become concentrated in Cannabis extracts. The process of making a Cannabis concentrate can elevate contaminants like pesticides as much as 5 to 10 times the concentration found in the Cannabis flower[8], meaning that if you are consuming a Cannabis concentrate, you are potentially being exposed to much greater doses of contaminants than if you were consuming the Cannabis flower used to produce that concentrate. I also want to point out that it’s not enough to simply test Cannabis flower for contaminants prior to making a concentrate. It is possible for there to be very trace amounts of pesticides or other contaminants present in the flower that won’t show up on a standard contaminant screening – but when concentrated they suddenly become present in dangerous levels.
n
[BACK TO ANTHONY SMITH SEGMENT]
n
The leaching of contaminants[9] [10] from cultivation, processing or packaging equipment is an issue that people working in the natural products industry have had to think about for quite some time. However some Cannabis companies are still learning about typical herbal processing and manufacturing best practices – putting consumers at risk. I spoke with Travis Simpson, an herbal scientist that has spent the past several years working with hemp in the Cannabis industry. He shared some of his concerns regarding contaminants from manufacturing and packaging equipment.
n
[TRAVIS SIMPSON SEGMENT]
n
One of the important things to note regarding most of these contaminants, including pesticides, metals, and mycotoxins, is that you won’t necessarily have an immediate reaction when you are exposed to these toxins. They can build up in the body over time, and you may not exhibit any symptoms for a long time before the body finally reaches a tipping point.[11] So just because you may have consumed a Cannabis product and didn’t notice any adverse effects, that does not mean that you are not being exposed to harmful contaminants.
n
The takeaway from my discussions was clear – know the purity of your Cannabis before consuming. But this is easier said than done. There are still many places in the US and abroad that have not legalized Cannabis or established strict testing requirements for Cannabis.[12] For users getting their Cannabis from the black market, they are left at the mercy of their supplier’s quality.
n
Unfortunately, this can sometimes lead to tragic consequences.
n
[ETHAN RUSSO SEGMENT]
n
Dr. Russo is referring to a recent string of fatalities linked to lung infections or lung damage associated with vape pens.[13]
n
[“VAPE CRISIS” NEWS REEL]
n
At the time of this recording, there have been 29 recorded deaths, and over 1300 reported cases of lung infections or damage linked to vape pens[14]. And these reports are growing at a rapid rate. While the exact culprit responsible for these illnesses and deaths has not yet been identified, investigators suspect it has to do with additives or contaminants.
n
[CONTINUE ETHAN RUSSO SEGMENT]
n
There is other evidence that contaminants in Cannabis have caused very serious problems for some people, which in rare cases has led to death. There are several case studies available of patients that contracted fatal lung infections, such as a condition called aspergillosis.[15] [16] Aspergillosis is a condition where the spores of certain species of Aspergillus fungi get nestled in small scrapes and crevices in the lungs where they begin to grow, forming a fungal mass called an aspergilloma[17]. This ultimately starts to break down lung function and can be fatal. In some fatal aspergillosis cases reported, contaminated Cannabis was deemed to be a contributing factor, and possibly the sole cause.[18]
n
This is more common in immunocompromised users than regular healthy users, but that just highlights the tragedy here. Many people with serious health conditions are turning to Cannabis as a medicine – and those patients are the ones most vulnerable to the adverse health effects of consuming contaminated Cannabis.
n
So let’s review what we’ve learned so far:
n
-
- n
-
- There are a lot of different contaminants that can appear in Cannabis and Cannabis products such as pesticides, residual solvents, metals, mycotoxins, molds, and bacteria.
n
-
- Metals and molds tend to appear most frequently in Cannabis flower, however metals do sometimes show up in extracts due to leaching from incompatible packaging
n
-
- Bacteria tend to appear most frequently in Cannabis infused products.
n
-
- Pesticides, solvents, and mycotoxins are more common in Cannabis extracts, because the process of making a concentrate actually concentrates these contaminants.
n
-
- Contamination is not always direct. Contamination can come from contaminated soil, water, drift from nearby farms, leaching from manufacturing equipment or packaging equipment.
n
-
- Contaminants or toxic additives have been responsible for fatalities associated with Cannabis consumption. Users with compromised immune systems are the most at risk.
n
n
By now we seem to be getting a pretty good picture about the safety profile of Cannabis. But we’re not done yet. There is one more issue that we haven’t discussed yet – and that’s adolescent Cannabis use. What unique risks might young Cannabis users face?
n
Find out in the third and final part of this series where we finish our curious quest to discover, “Is Cannabis Safe?”
n
[OUTRO MUSIC]
n
n
Citations and Resources
n
[1] “#01 Is Cannabis Safe? Part One”. The Curious About Cannabis Podcast. Natural Learning Enterprises. 2019. https://cacpodcast.weebly.com/episodes/01-is-cannabis-safe-part-one
n
[2] How Pesticides Work. Kentucky Pesticide Safety Education Program. http://www.uky.edu/Ag/Entomology/PSEP/12pesticides.html
n
[3] Kim et al. Exposure to pesticides and the associated human health effects. Science of the Total Environment. 2017. 575(1): 525-535.
n
[4] https://www.nbcnews.com/health/vaping/tests-show-bootleg-marijuana-vapes-tainted-hydrogen-cyanide-n1059356
n
[5] Product Safety Assessment: Myclobutanil. Dow Chemical. http://msdssearch.dow.com/PublishedLiteratureDOWCOM/dh_08d6/0901b803808d60fd.pdf?filepath=productsafety/pdfs/noreg/233-01023.pdf&fromPage=GetDoc
n
[6] Pond SM, Tozer TN. First-pass elimination. Basic concepts and clinical consequences. Clin Pharmacokinet. 1984. 9(1): 1-25.
n
[7] Huestis MA. Human Cannabinoid Pharmcokinetics. Chem Biodivers. 2009. 4(8): 1770-1804.
n
[8] Voelker R, Holmes M. Pesticide Use on Cannabis. Cannabis Safety Institute. 2015. https://cannabissafetyinstitute.org/wp-content/uploads/2015/06/CSI-Pesticides-White-Paper.pdf
n
[9] https://www.coleparmer.com/chemical-resistance
n
[10] https://www.scilabware.com/en/chemicalcompatibility/
n
[11] Williams et al. Human aflatoxicosis in developing countries: a review of toxicology, exposure, potential health consequences, and interventions. The American Journal of Clinical Nutrition. 2004. 80(5):1106-1122.
n
n
[13] https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html
n
[14] https://www.sciencenews.org/article/vaping-tied-nearly-1300-lung-injuries-29-deaths-united-states
n
[15] Gargani et al. Too Many Mouldy Joints – Marijuana and Chronic Pulmonary Aspergillosis. Mediterr J Hematol Infect Dis. 2011. 3(1): e2011005.
n
[16] Ruchlemer et al. Inhaled medicinal cannabis and the immunocompromised patient. Support Care Cancer. 2015. 23(3):819-822.
n
[17] https://www.mayoclinic.org/diseases-conditions/aspergillosis/symptoms-causes/syc-20369619
n
[18] Gargani et al. Too Many Mouldy Joints – Marijuana and Chronic Pulmonary Aspergillosis. Mediterr J Hematol Infect Dis. 2011. 3(1): e2011005.
n
Podcast: Play in new window | Download
Subscribe And Never Miss an Episode! Apple Podcasts | Google Podcasts | Spotify | RSS | More